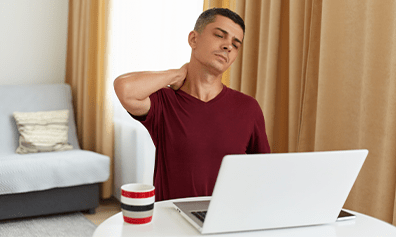
Tailbone Pain-
Does your job demand you to sit for long hours in front of your computer? Do you sit at your workstation for seemingly endless hours?
If yes, then you most probably what this pain feels like. The tailbone pain, also known as coccydynia, is pain and tenderness at the tip of your tailbone, the area between the buttocks. Although mostly an occupational hazard, it can also be caused by falls, any injury, or during childbirth. The Study A study done on 2000 cases of back pain referred to hospital stated nearly 2.7% were diagnosed as coccydynia [1]. This pain occurs five times more frequently in women than in men. It can occur at any age, but the mean age of onset is around 40 years [2].The most common symptoms are:
- • Pain in the tailbone, that may get worse with sitting or leaning back against something
- • Tenderness and redness in the affected area
- • Discomfort during bowel movements
- • Difficulty in standing from resting position
the things that can help you get rid of your tailbone pain:
- •Avoid any strain or re-injury in the area of constant pain
- • Avoid sitting for a long time in the same position
- • Sitting on hard surface on daily basis can trigger the pain, please avoid
- • Use a cushion specially designed for coccydynia
- • Use OTC pain pills for severe pain
- • Eat healthy fibers to avoid applying pressure during bowel movements
- • Posture correction is very important, sit in a way to avoid overpressure on your tailbone
- • Exercising regularly for at least 30 minutes is very important. Jogging and walking are the best options
- • Physical therapy can help you overcome your tailbone pain. Ultrasonic massage can also be helpful
- • Surgical intervention can be recommended in unresponsive cases
- Ghormley RK (1958). "An Etiologic Study of Back Pain". Radiology. 70(5): 649–653.
- Patel, R; Appannagari, A; Whang, P.G. (May 2008). "Coccydynia". Current Reviews in Musculoskeletal Medicine. 1(3–4): 223–226. doi:1007/s12178-008-9028-1. PMC 2682410 . PMID 19468909.
Various approaches employing physical therapy, ergonomic adaptations, medications, injections, and, possibly, psychotherapy lead to greater chances of success in patients with refractory coccyx pain. Conservative treatment is successful in 90% of cases. Although new surgical techniques are emerging, more research is needed before their efficacy can be established. Its prognosis is good and the patient can recover fully but this condition can reoccur if precautions are not taken. So, stop ignoring your pain, as now you can get treated right from your home after work conveniently and effectively
REFERENCES